

Robotic surgery is the newest tool in the armamentarium of a Minimal access surgeon. Though in its infancy, it is fast developing as a very useful modality especially in fields like gastrointestinal surgery, urology and thoracic surgery. It’s excellent visualisation and handling capability allows it to be very handy in places of difficult surgical access . High above and down low in the abdomen are two such places where extreme dexterity is required and the robot comes in handy. Robotic surgery has established itself in fields like bariatric surgery and colorectal surgery. It is extensively used in surgery for both benign and malignant colorectal diseases such as rectopexy, resections, low anterior resection and abdominoperineal resection. Robotic surgery has of late also progressed to surgeries for esophagus , pancreas and hepatobiliary systems. We have been using the robot for our various upper and lower gastrointestinal tract surgeries.
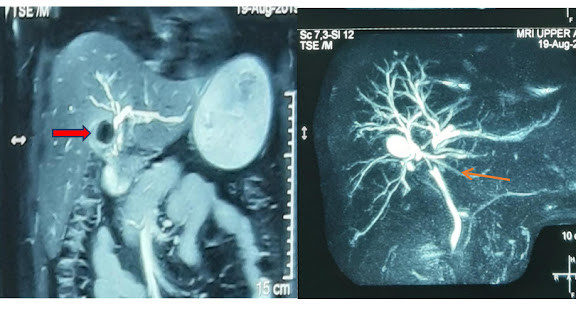
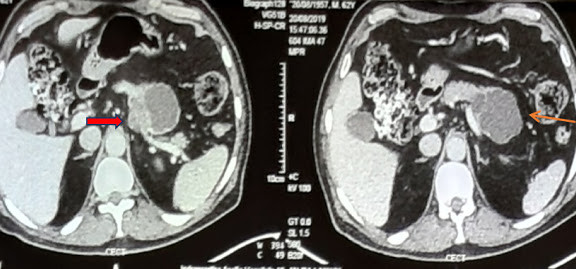
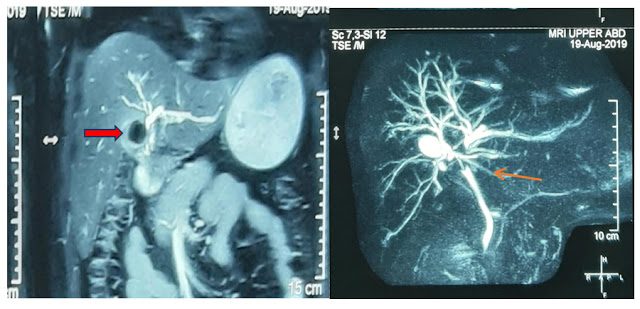
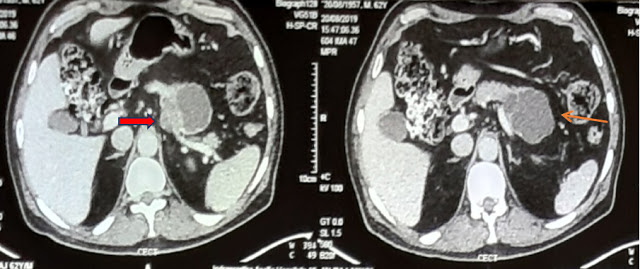
Here we present an interesting rare case operated by us using robotic technology. The patient was a middle aged lady with history of dysphagia (difficulty in swallowing food ) since past 2 months. On investigation she was found to have a large epiphrenic diverticulum ( outpouching from the lower end of esophagus). She was investigated by barium swallow, CT abdomen and oesophageal manometry. No other motor abnormality was noted in the oesophageal musculature. She was planned for Robotic excision of epiphrenic diverticulum. The case was prepared with all necessary investigations and clearances.
She was operated from the abdomen using the daVinci robotic system. 5 ports were used including one for the camera and an extra port for liver retraction. After dissecting the hiatus and skeletonising the diverticulum, the oesophagus was intubated with a 52 fr bougie. A linear stapler was fired on the mucosal diverticulum after ensuring adequacy of the oesophageal lumen. The integrity of the transection line was checked with dye test.
She tolerated the procedure well. Post operatively the patient was started on oral liquid diet on POD 1 after removal of Ryle’s tube . She was subsequently discharged on Pod 4 after removal of abdominal drain.
Presently she is 2 months post procedure and is tolerating liquid and soft diet comfortably without any dysphagia. Traditionally if the same surgery would have been performed it would have resulted in a prolonged recovery in view of the large surgical incision. We were able to provide such a fast recovery to this patient because of the assistance of the robot.
We thus believe that Robotic surgery is an extremely safe and easy modality in the armamentarium of a surgeon. It allows meticulous dissection by way of its better visualisation and surgical dexterity.There is an amazing scope for this modality of surgery in the future.
{kind=link}
{kind=link}
{kind=link}